
The first hip arthroscopy was performed in Nashville in 1990. Dr. Byrd was asked to evaluate a teenage boy with loose fragments in his hip left over from a previous fracture of the acetabulum (hip socket). Traditionally, removal of these would require a large open incision with dislocation of the hip. It seemed to make sense to try to tackle this arthroscopically to avoid the potential problems associated with such a large open operation. Dr. Byrd employed the basic arthroscopy principles he used in other joints, such as the knee, shoulder, and elbow, taught to him by his mentor Dr. James Andrews. He removed the loose bodies, and it worked.

Dr. Byrd with his mentor Dr. James R. Andrews, covering a football game in 1987.
Over the next couple of years, he removed a few more loose bodies on patients referred to him. (Related Study: Hip arthroscopy for posttraumatic loose fragments in the young active adult: three case reports) At that time, these were really the only things that were being diagnosed as a cause of hip problems that could be addressed with arthroscopic surgery. Loose bodies could be seen on x-rays, and back then, MRIs commonly used today for diagnosing other problems were still in their infancy.
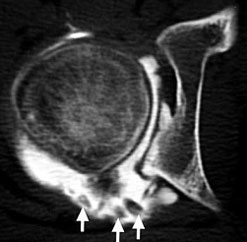
Dye inside the joint silhouettes the loose bodies (arrows).

Arthroscopic view of the loose bodies.
A video of this first arthroscopic removal of loose bodies.
16 year old boy with bony loose bodies in his hip. Arthroscopy was tried as an alternative to a major open operation with successful removal.
In 1992, he operated on a patient with a fourteen year history of locking, catching, and giving way of his hip for what sounded like loose bodies, although none could be seen on his studies. During arthroscopy, he was found to have a large, torn fragment of his labrum catching within the joint, and this was removed. The patient experienced immediate resolution of his symptoms and actually continued to do well almost twenty-five years later. This is when it became evident that there were other problems inside the joint, such as labral tears, that could cause significant problems.

X-rays and other studies did not detect the tear.

A quarter of a century later the patient’s X-rays are still normal and remains pain-free.
Watch the surgery, which revealed and treated the torn laburm.
1992, first Hip Arthroscopy performed for a Labral Tear, with debridement of a large entrapped fragment.
In 1994, Dr. Byrd published the landmark article Hip Arthroscopy. The Supine Position., describing the technique that he developed; and this has subsequently been adopted worldwide as the most common method for performing hip arthroscopy. (Related Study: Hip arthroscopy utilizing the supine position) In 1995, his study describing the anatomy of the structures around the hip during arthroscopy was the first scientific paper ever accepted for presentation at the American Academy of Orthopaedic Surgeons (AAOS) Annual Meeting. In 1996, he published his early observations on labral tears, defining some of the common patterns as we know them today. (Related Study: Labral lesions: an elusive source of hip pain case reports and literature review)
In 1997, Dr. Byrd gathered with Dr. Howard Sweeney at the Orthopaedic Learning Center in Chicago and devised a method for practicing hip arthroscopy on cadaver specimens so they could teach others how to perform this procedure. Later that same year, they inaugurated the first motor skills course on hip arthroscopy in Chicago. Early on, this was the only annual site for teachers and students alike to gather to share knowledge on the gradually advancing principals of hip arthroscopy. These courses continue today and have been the model for the now hundreds of programs available around the world.
Also in 1997, Dr. Byrd performed the first arthroscopic hip procedure ever carried out on an NFL football player; setting the stage for hip arthroscopy in professional athletes. Subsequently, in 2001, Dr. Byrd published the first scientific article on hip arthroscopy in athletes, defining its efficacy for the problems that were known in that day. (Related Study: Hip arthroscopy in athletes)

Dr. Byrd and Howard Sweeney test a device for holding a cadaver specimen in preparation for the world’s first motor skills course for surgeons.
The first arthroscopic procedure ever performed on an NFL professional football player. Twenty years later, his hip is still holding its own.
2003 was a landmark year. Dr. Byrd first met Professor Reinhold Ganz from Bern, Switzerland, when they spoke together on a program in Helsinki, Finland. In that same year, Professor Ganz published his landmark article on femoroacetabular impingement (FAI) as a cause of osteoarthritis. For arthroscopic surgeons, it quickly became evident that this FAI was a cause of many of the joint problems that were being encountered long before the patients or athletes actually developed osteoarthritis.
This was a game changer for the role of arthroscopy. Now surgeons could start to identify and treat the underlying etiology in addition to addressing the damage it caused. Early debridement procedures evolved into restorative operations, reshaping the bone to correct the FAI and repairing the labrum and other structures to provide more durable, long-term results.

Dr. Byrd and Professor Ganz lectured together in Helsinki in 2003.
Through teaching these methods to others, the small band of early pioneers has now grown to a large group of innovative, talented surgeons, clinicians, and scientists. This has led to an exponential proliferation in understanding a variety of hip disorders and concomitant strategies for their treatment. Much of this is steered through the International Society for Hip Arthroscopy (ISHA), founded by Dr. Byrd and others in 2008.

The birth of ISHA with its Founding Members in Paris, France, 2008
With better understanding and early recognition, it is now possible to emphasize the role of prevention and conservative care in addition to advanced strategies in surgical management. This involves not only the hip joint, but numerous other structural problems around the joint as well, including tendons and bursas and nerves. Many can be addressed with less-invasive arthroscopic techniques, but some still require the role of open surgery for the most predictable results. Thus, treatment always requires a comprehensive team approach to customize the correct care path for each individual. Today’s team includes nurses, mid-level providers, physical therapists, physicians skilled and knowledgeable in both nonsurgical and surgical management and, when needed, a complete surgical team. All are important to insure the most successful surgical outcome.
Location
2004 Hayes Street
Suite 700
Nashville, TN 37203
Office Hours
Monday-Friday:
8:00 am – 5:00 pm